9 Letter Medical Necessity Template
B 12 months from the date of the first service associated with the letter. Sample letter template of medical necessity for astellas products to prescriber.
 Sample Letter Of Medical Necessity
Sample Letter Of Medical Necessity
Patient letter of medical necessity.

Letter medical necessity template. To be completed by employee. Template for a letter of medical necessity and statement form. The letter should be written on official letterhead with complete contact details.
A new letter will be required to document claims incurred after the expiration of the letter. Cancer medical necessity letter template. Please refer to the important safety information in the full prescribing information including any boxed warning when determining whether therapy is medically appropriate for the individual patient.
Date payer name payer address attn. The following content can be cut and pasted onto your practices letterhead and used as a letter of medical necessity. North chicago il 60064 us abbv 190416 december 2019 printed in usa.
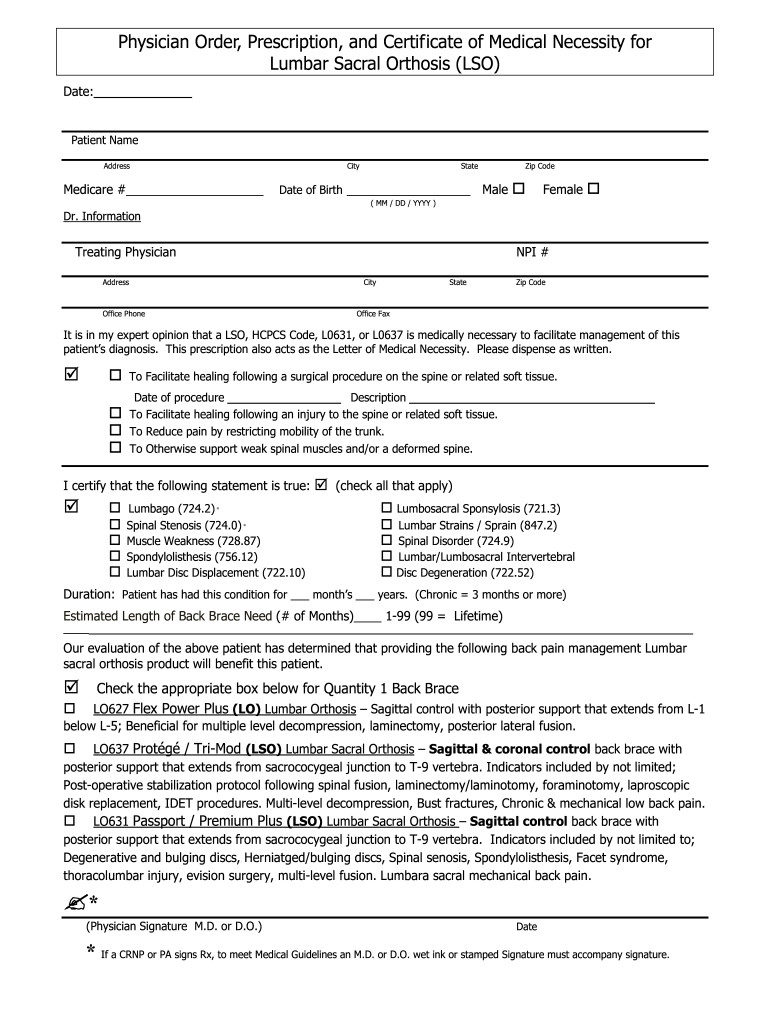
Provide a brief background of the patients medical history including past treatmentsmedicationsequipment. Treatmentmedicationequipment item in questionfor the treatment of specific diagnosis. Detail the patients diagnoses.
Medical director health plan address. Or c the end of the duration of treatment. Sample letter of medical necessity.
I am writing on behalf of my patient patient nameto document the medical necessity of. A prior authorization allows the payer to review the reason for the requested therapy and to determine medical appropriateness. A letter of medical necessity will expire upon the earliest of a 12 months from the date of the letter.
Comprehensive evaluation letter of medical necessity. You may customize a letter of medical necessity template the way you deem correct there is no uniform format and as long as this document contains all important details about the patients health condition and you offer the recipient a chance to contact you and know more this statement will be accepted and reviewed. Sample letter of medical necessity 2019 abbvie inc.
This letter provides information about the patients medical history and diagnosis and a statement summarizing my treatment rationale. Patient name policy idgroup number date of service to whom it may. Letter of medical treatment.
Sample letter of medical necessity. Sample letter of medical necessity for dupixent dupilumab this letter provides an example of the types of information that may be provided when responding to a request from a patients insurance company to provide a letter of appeal for dupixent. The statement of medical necessity form is attached for your use at your discretion.
Replacement device letter of medical necessity. Free 20 medical necessity letter templates in pdf ms word. Medical diagnoses icd 9 codes.
Sample letter of medical necessity payers may require prior authorization or supporting documentation in order to process and cover a claim for the requested therapy. Letter of medical necessity.
Letter Of Medical Necessity Eleven Point Checklist Template
 Template Letter For Medical Necessity
Template Letter For Medical Necessity
Sample Letter Of Medical Necessity Manual Hospital Bed
 Sample Letter To Doctor For Treatment Top Form Templates
Sample Letter To Doctor For Treatment Top Form Templates
Bath Lift Letter Of Medical Necessity Sample J T Physician
Sample Letter Of Medical Necessity Sample Letter
 Pin On Free Tamplate
Pin On Free Tamplate
 Medical Necessity Form Fill Out And Sign Printable Pdf Template Signnow
Medical Necessity Form Fill Out And Sign Printable Pdf Template Signnow
Belum ada Komentar untuk "9 Letter Medical Necessity Template"
Posting Komentar